
- Case Studies
How Better Mental Health Care Transitions Lower Readmission Costs
Discover how Georgia and Florida’s Mental and Behavioral Health Center tackled rising readmission rates and costs with strategic staffing and care transitions.
Table of Contents
Introduction
Nationwide, hospitalizations for mental health disorders have surged, surpassing all other conditions. A pressing concern is the lack of timely bed space for these patients. Georgia notably closed over half its state psychiatric beds in 2021-2022.
- Mood disorder patients face a 15% readmission rate within 30 days, while schizophrenia patients experience an alarming 22.4% rate.
- The average U.S. readmission cost is approximately $7,200, but the greater concern lies in poor patient outcomes due to limited access to community mental health resources and care plan adherence issues, fostering chronic relapses.
Elevated Readmission Rates for Mental Health Patients
On a national scale, hundreds of thousands of individuals seeking mental health care rely on local hospitals. In 2021,
- Inpatient admissions for mood disorders surged to 847,000, while those for schizophrenia, one of the most severe mental illnesses, reached 383,000.
- By 2022, it was estimated that 37 percent of individuals with disabilities on Medicare were contending with serious mental disorders.
Both mood disorders and schizophrenia are associated with higher readmission rates, compounding the pressure on already limited inpatient mental health treatment resources.
- Nationally, 15 percent of patients with mood disorders are readmitted within 30 days, while the rate for patients with schizophrenia stands at a staggering 22.4 percent
- By 2022, it was estimated that 37 percent of individuals with disabilities on Medicare were contending with serious mental disorders.
- The U.S. faces an average cost of approximately $7,200 for each subsequent hospital stay.
Key factors driving this cycle of readmission encompass issues related to
- Medication Management
- Suboptimal Outpatient Follow-up
- Co-occurring Substance Use Disorders.
The Mental and Behavioral Health Center operates as an integrated delivery system, providing inpatient and outpatient mental health care across communities in Georgia and Florida.
Acknowledging the vulnerability of patients with mood and mental health disorders to readmission, the center is steadfastly committed to enhancing outcomes for this demographic.
Strained Resources Hinder Continuous Treatment
At the Mental and Behavioral Health Center, the acuity levels of mental health patients have been on the rise, while inpatient and outpatient services are stretched increasingly thin. In the state of Georgia,
- Over 50 percent of available state psychiatric beds were shuttered
between 2021 and 2022.
Furthermore, Georgia faces a shortage of psychiatrists compared to other states, and access to essential outpatient resources such as crisis stabilization and rehabilitation services has become progressively challenging.
This shortage of both inpatient and outpatient mental health services has culminated in an influx of patients seeking mental health care at emergency departments (ED), where many are held for extended periods as they await the availability of inpatient beds or outpatient services.
Post-discharge, a considerable number of patients experience no contact with their outpatient mental health providers for weeks or even months.
The establishment of case management services for patients with complex mental health needs can take up to 60 or even 90 days as referrals traverse the approval process.
With these sobering challenges as the backdrop, the Mental and Behavioral Health Center embarked on a mission to enhance outcomes for patients grappling with mental illness.
This included a determined effort to lower readmission rates and facilitate greater access to community support. The center’s strategy revolved around optimizing care planning within inpatient mental health units, ensuring a seamless transition to successful outpatient treatment.
The Solution
To address these challenges, we collaborated with the Mental and Behavioral Health Center to implement a transformative care transition process, involving workflow redesign and key patient support roles. To assess these changes, The center utilized our cutting-edge Analytics Platform, integrating AI and automation solutions and a comprehensive suite of analytical applications.
Elevating Mental Health Care Transitions
To realize these objectives, the Mental and Behavioral Health Center recognized the imperative of strengthening collaborations with external organizations while introducing novel roles and interventions internally. The latter necessitated a workflow redesign, underpinned by robust data and analytics for monitoring the effectiveness of the implemented measures.
Piloting a refined transition process, the Mental and Behavioral Health Center secured a grant to launch an enhanced care transition project in partnership with Medientsky Billing, serving patients across seven different states.
This initiative encompassed five outpatient mental health agencies, collectively providing a comprehensive treatment approach for individuals grappling with severe and persistent mental illnesses, co-occurring substance dependency, chronic health conditions, and socioeconomic challenges.
The primary objective of the project was to extend access to community support for adult mental health inpatients at the highest risk of readmission. This was achieved by developing and implementing a collaborative discharge and transition pilot, with the core aim of reducing readmissions by at least 10 percent.
The project team worked diligently to:
- Develop mental health interventions to enhance the likelihood of successful recovery in the outpatient setting, ultimately reducing readmissions.
- Augment access to community mental health resources while patients were still in the hospital.
- Created a patient-centered recovery model that encourages early patient and family engagement in discharge planning.
- Enhance patient advocacy in treatment and demonstrate improvements in the patient experience.
- Improve communication between inpatient and outpatient resources to ensure seamless care transitions and follow-up.
In addition to monitoring process metrics tied to the recovery plan and outreach, the readmission rate was established as the paramount performance indicator.
Optimizing the EHR for Robust Documentation and Analytics
The Mental and Behavioral Health Center underwent a comprehensive revision of its Electronic Health Records (EHR) system to fortify
- Documentation of community care coordination
- Transition meetings,
- Follow-up appointments,
- Discharge record transmission
- Goal-setting meetings involving patients and their families.
Subsequently, the center harnessed our Analytics Platform, integrating AI and automation solutions with a wide-ranging suite of analytical applications, to aggregate data from the EHR.
This platform equips the Mental and Behavioral Health Center with the capability to oversee and assess both the care process and outcome measures.
Engaging Patients and Fostering Trust
Two pivotal roles were introduced at the Mental and Behavioral Health Center to support a successful transition and activation of outpatient resources: the mental health navigator and the peer support specialist.
The mental health navigator, a mental health professional, collaborates closely with patients and the care team to establish vital outpatient services, enhance discharge planning, advance patient-centered recovery initiatives, and conduct routine outpatient follow-ups with both contacts and patients. The peer support specialist, an individual with a mental health diagnosis who has successfully navigated recovery for at least one year and obtained peer support specialist certification, serves as the patient’s advocate. They foster a trusting relationship with the patient, engage in or lead recovery groups, motivate patients to participate actively in care planning, and deliver an outpatient follow-up to sustain recovery and avert crises as necessary.
Proactive Patient Engagement
With these roles in place, the Mental and Behavioral Health Center undertook a comprehensive redesign of the inpatient workflow. Upon admission, the social worker conducts a diagnostic assessment, while the mental health navigator evaluates every adult patient to determine their eligibility for the pilot program. The criteria for pilot inclusion include residing in the metropolitan area, a high risk of readmission due to a diagnosed condition, previous hospitalization or visits to the emergency department for mental health concerns, and a lack of available outpatient services. Patients meeting these criteria are invited to participate in the program by the mental health navigator. In cases where patients decline participation, the peer support specialist engages with them to encourage involvement in the program—a rare occurrence during the pilot. Participating patients sign a release of information form that remains in effect for five years from the date of signing, facilitating continuous bilateral exchange of patient information between the Mental and Behavioral Health Center and the five participating agencies. This ensures that communication between the mental health experts in the hospital and the community persists even after the patient’s discharge.
Efficient Care Coordination
The mental health navigator identifies unique patient needs and dispatches referrals for community services to a community hub via a service request. The community coordinator reviews the service request and shares it with the five outpatient mental health agencies.
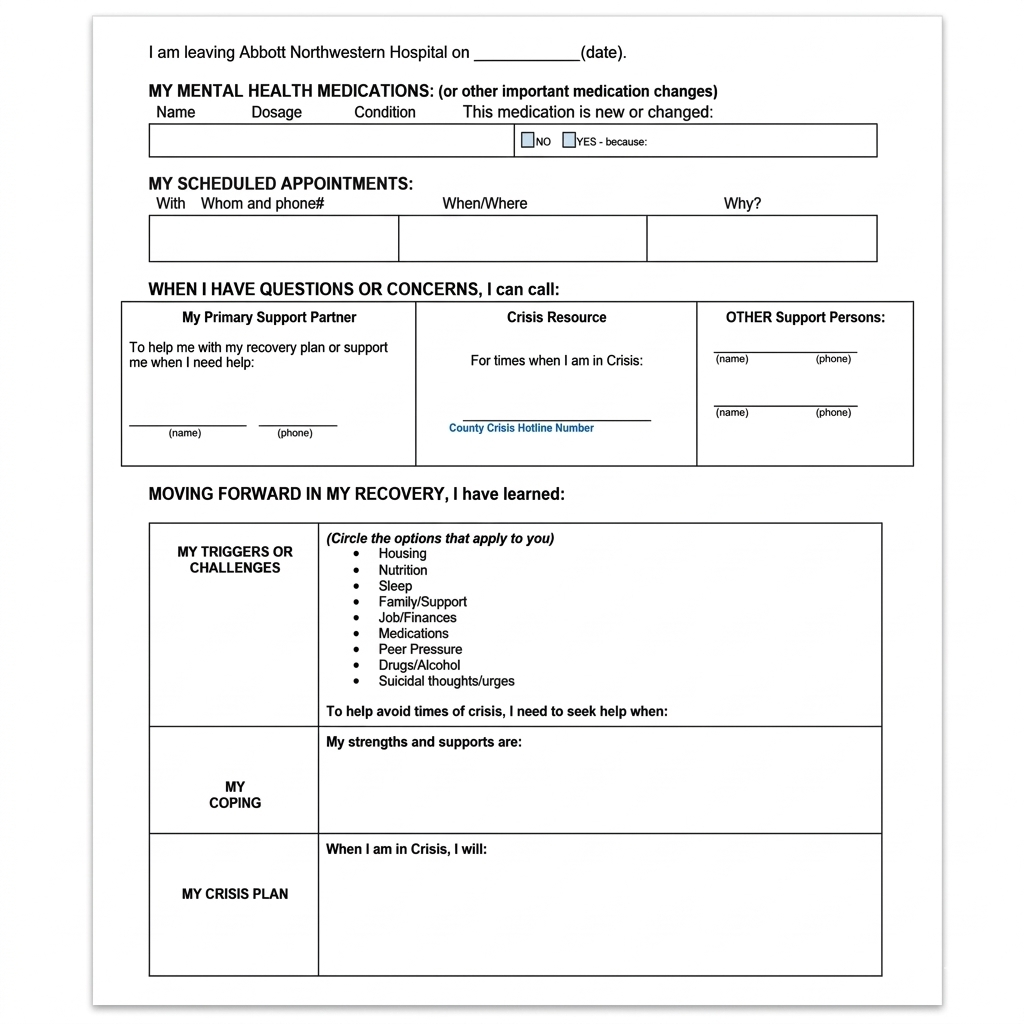
These agencies evaluate the patient’s requirements and respond within 4-6 hours, if not sooner, with the resources they can offer. The mental health navigator reviews these options with the patient, and in collaboration with the community coordinator, identifies the agency best suited to meet the patient’s needs. Prior to discharge, several critical actions are taken. Firstly, the selected agency is contacted to initiate an on-site assessment and develop an early outpatient plan while the patient is still hospitalized. This proactive engagement helps eliminate delays in establishing timely and effective outpatient care while enhancing the building of relationships that bolster the likelihood of ongoing patient engagement in services after discharge. For many patients, the contacts occur on-site for multiple visits, particularly if their care is highly complex. Secondly, prescriptions required post-discharge are filled at the hospital to increase the likelihood of medication adherence in the outpatient setting. Pharmacy educators offer group educational sessions to review the significance of medications, and potential side effects, and address any patient queries. Thirdly, patients take part in transition meetings, plan for discharge, set goals, and establish their recovery plan. This Recovery Plan is crafted in collaboration with the patient early in the admission process and is articulated in patient-centered, easy-to-understand language.
Sample Patient-Centered Recovery Plan
Following the patient’s discharge, records related to their inpatient stay and post-discharge needs are promptly transmitted to the next level of care, ensuring a seamless transition within 24 hours. The agency’s commitment to patient well-being is evident as they make contact with the patient within 48 hours after discharge, often extending their support by reaching out to the patient on the very day of their release. Both the mental health navigator and the peer support specialist continue their invaluable support after discharge. Between 30 to 45 days following discharge, they arrange a follow-up phone call with the agency contact and the patient to review their recovery status and explore opportunities to enhance outpatient care. The effectiveness of a collaborative team approach becomes evident when patients encounter challenges while receiving outpatient care. In such instances, the agencies can readily engage the mental health navigator and mental health experts for assistance. In a particularly compelling case, a patient in the outpatient setting fell victim to a robbery, resulting in the theft of their medications. Given that the prescription had been filled within the last 30 days, insurance coverage was initially denied for a refill. The agency promptly reached out to the mental health navigator, who coordinated with inpatient mental health prescribers and pharmacy staff. The team’s collective efforts extended to contacting the insurance company, eventually securing coverage for the medication refills. This ensured that the patient could adhere to their prescribed regimen, thereby averting an unnecessary readmission. In another instance, a patient was discharged to a chemical dependency treatment program but was subsequently removed from the program, putting her at risk of violating probation and potential incarceration. The patient sought assistance from the navigator, who helped her locate a crisis residence, enabling her to remain compliant with the terms of her probation and avoid incarceration. Yet another remarkable example features a 22-year-old homeless man who had been admitted multiple times for chemical dependency issues and a suicide attempt. He began working with the peer specialist and was discharged to a faith- based treatment facility for one-year outpatient treatment, in line with his preferences. The peer specialist maintained frequent contact with the patient, establishing a supportive relationship and aiding the patient in his recovery journey. Today, this same individual is actively pursuing a career as a peer support specialist, undergoing the training that will enable him to help others facing similar challenges in the future.
Results
The enhanced care transitions program at The Mental and Behavioral Health Center is yielding significant improvements in patient care transitions while effectively reducing readmission rates in the field of mental health.
- A remarkable 27 percent relative reduction in potentially preventable readmission rates stands out as one of the program’s key successes.
- When compared to a control group, patients benefiting from enhanced care transitions exhibited significantly lower readmission rates.
- On a national scale, the 30-day readmission rate for patients with mood disorders typically hovers around 15 percent, whereas for patients with schizophrenia, it reaches 22.4 percent.
- In stark contrast, the enhanced care transitions program has achieved a remarkably low readmission rate of just 4.6 percent within 30 days.
Furthermore, the program has realized a remarkable 97 percent relative improvement in the timely transmission of records within 24 hours following discharge. Multiple aspects of patient care have also witnessed improvements, including:
- 95% Of patients now have a carefully constructed recovery plan.
- 90% Of patients are efficiently linked with the
- 88% Of patients receive an onsite agency visit before discharge.
- 94% Of patients are scheduled for a follow-up appointment before discharge.
- 100% Of patients receive a closed-loop call within 45 days post-discharge
- 92% Of patients successfully arrive at their follow-up appointments
While two patients faced incarceration and were unable to attend their follow-up appointments, one patient requested a different psychiatrist and had their appointment rescheduled.
Conclusion
Most notably, the program boasts an impressive patient retention rate exceeding 80 percent. This remarkable achievement exceeds national retention rates and underscores the program’s ability to effectively retain patients within established outpatient services for a month post-discharge.
Share it on
Search Latest Case Studies
Highlights
- 60 or even 90 Days referral process
- 30-day Readmission rate for patients
- 4-6 hours, Patient's requirements responds
Client Specs
- Location: Washington
- Specialty: Behavioral Health
- EHR: Incredible
- Average collections: 300K per month
Work with medical billers who understand your EHR's billing process backwards and forwards
Get paid Three times faster with our 24/7 medical billing services.
Avail Free RCM Audit Worth $2,000! Check out 19 different KPI reports that stops your cash flow.